Data in Action with Zanzibari Local Government
 |
May 07, 2018
|
May 07, 2018
Through our Safer Deliveries program, D-tree works closely with the Zanzibar Ministry of Health to develop a culture of data use and action.
Ready, set, action! Our dashboards help the Zanzibari local government take action to improve maternal and newborn health in their districts. In January 2018, we saw five District Health Management Teams (DHMTs) present on “action plans” based on dashboards at the Saving Lives at Birth funded Safer Deliveries program Quarterly Review Meeting.
Ministry of Health (MoH) and local government involvement is one critical success factor for the Safer Deliveries program, a collaborative initiative between the Zanzibar Ministry of Health and D-tree International. This program, implemented at scale in ten of Zanzibar’s eleven districts, trains community health volunteers (CHVs) to work with the aid of digital tools to deliver maternal and newborn care and to encourage facility-based deliveries.
As a by-product of the care given, the Ministry and DHMTs obtain high-quality data in quasi-real-time, which builds the government’s capacity to analyze the data and improve their decision-making. DHMT dashboard-based action plans are one way that the Safer Deliveries program is building policy-makers’ capacity to analyze and utilize data for decision-making. We trained DHMTs to analyze dashboards, identify areas of concern, and create an “action plan” to follow up on their concern, better understand the issue at hand, and seek resolution.
As we worked with DHMTs, we followed the following process to ensure the government has the capacity and tools to succeed: designing dashboards with the user, building capacity through tools orientation, and providing follow up.
1. Design for the user, with the user

To ensure dashboards were useful for DHMTs, we designed with the end users and worked with them to determine what is most relevant to the DHMT role as district health decision makers. We worked with MoH staff and DHMTs throughout dashboard design and after development.
-
During the design phase, we met with MoH staff to review the existing dashboard and highlight data points that we thought would be most useful to DHMTs, such as information about antenatal visit payments, home deliveries as well as perinatal deaths. This is relevant for DHMTs because they can then follow up on root causes of these problem areas. We also identified that dashboard graphs and tables should be as detailed as possible so that the data is meaningful for DHMTs and provides them with sufficient information so that they can take action at the district level.
-
After the dashboard was developed and before DHMTs created their action plans, we conducted at least two orientation sessions with each DHMT in which they reviewed the dashboards and gave us feedback on the design. As DHMTs reviewed the details of the dashboards in these sessions, we received important feedback on usefulness of dashboards and suggestions for improvement.
-
As the DHMTs developed their action plans, some individuals provided additional suggestions on design, often requesting that we add more detail. We made modifications accordingly so that DHMTs could be most effective in executing their action plans.

Another aspect we considered for the DHMTs was to avoid information overload. We collect hundreds of data points in the program as a by-product of the CHV-client interactions. There is an indefinite number of analyses that we could create to visualize this data, but when we are trying to support a culture of using data for decision-making, we have found that less is more. Finding the most high-impact and useful ways to describe specific data helps focus DHMTs’ attention on issues which they care about most, and which they can use to take action. This was an important consideration in our process and has led to dashboard content, which is specific, relevant, and actionable.
2. Orientation to dashboards and data

We oriented the DHMTs to the dashboard to ensure they had the skills and tools they needed to identify their concerns and take action. First, we oriented up to three members of each DHMT on the dashboard—the Reproductive and Child Health Officer, the Monitoring and Evaluation Officer, and the District Medical Officer. We helped them login to the dashboard, reviewed the data available, and helped them begin to identify problem areas, and how to analyze them. We then invited them to a follow up session to engage in a hands-on dashboard exercise. We provided each DHMT with a worksheet, which asked questions about certain data points and indicators available. DHMTs worked in teams to review the dashboard in order to answer the questions. This exercise helped to improve DHMTs ability to navigate the dashboard and peaked their interest in the data available.
3. Develop action plans
We provided each DHMT with action plan templates to help them document issue areas, propose actions to address the concerns, and track progress. First DHMTs reviewed the dashboard and documented five areas of greatest interest or concern. They justified why they selected each area of concern in order to relate the concern to a district priority or inconsistency with government policy, for example. Next, DHMTs made a plan of action—they specified the steps they plan to take to further explore the concern or address it in order to achieve improvements in health services.
DHMTs were pleased with the action-plan development process and said that it helped them to confidently document problems and track progress toward addressing the issues identified.
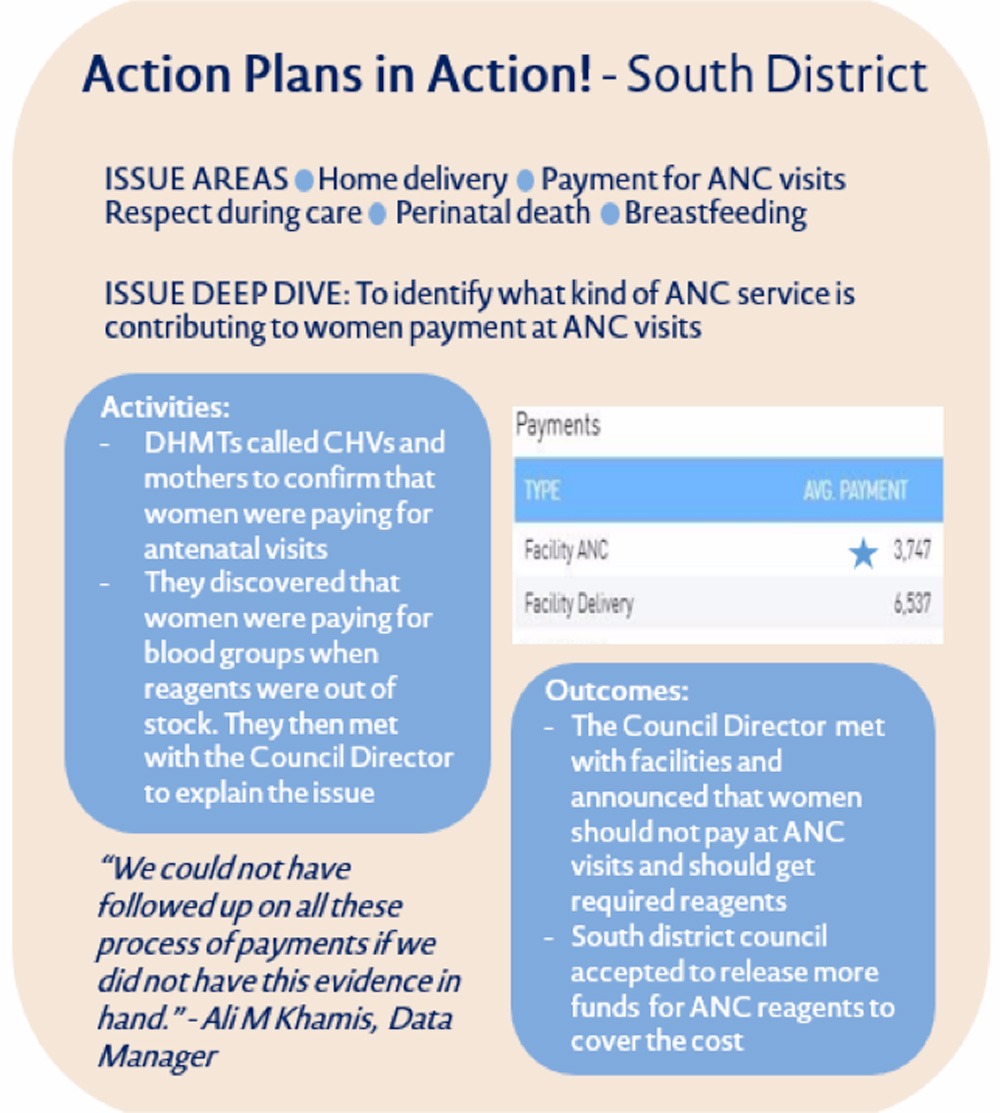
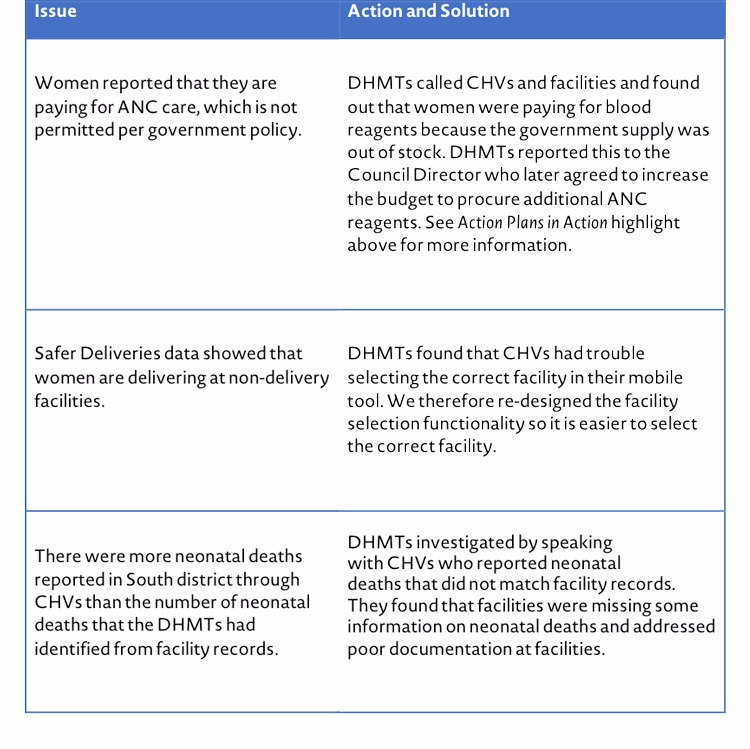
Some issue areas and solutions that came up from action plan activities include:
4. Follow up
As part of action plan execution, our team followed up very closely with DHMTs and called them every two weeks for two months to see how they were progressing with their action plan and to discuss if they were having any issues. We were available to provide technical support or additional information, as needed. DHMTs were excited to engage in addressing actions and concerns throughout this time. They found the actions valuable and directly related to their role, as well as their objectives to improve health in the district.
After the design, orientation, and follow up, DHMTs successfully presented the actions they had taken as part of their dashboard action plans. Meeting participants were impressed to see the deep engagement and investment of DHMTs. DHMTs appreciated having data at hand as they advocated for additional resources or explored concerns in their communities. The Safer Deliveries program is planning to have DHMTs devise and implement action plans on a quarterly basis. We will also work with the DHMTs to incorporate such activities into their 2018-2019 District Health Plans.
Ministry of Health and local government capacity to utilize data for decision-making is important for long term sustainability and success of the program. To date, this program has consistently shown 50% increases in facility delivery rates and four-fold increases in postpartum follow-up among women in the program. With activities like action plans, which methodically identify specific improvement areas, these outcomes will only get better. We are currently collaborating with the MoH Health Management Information Systems (HMIS) unit to integrate Safer Deliveries data into the Ministry’s new DHIS-2 based community health database to ensure data from the program is integrated into the Ministry’s systems. We will continue to work closely with national, zonal and district officials to support analysis and interpretation of this data for decision-making.